
Mesial Temporal Sclerosis (MTS)
What Is Mesial Temporal Sclerosis?

Mesial temporal sclerosis (MTS) is a term used to describe scarring in the deep part of the temporal lobe of the brain. MTS is the most common cause of structural epilepsy and focal seizures in the temporal lobe. MTS affects the hippocampus which is the brain region that is involved in memory formation and retrieval, and the amygdala which is involved in emotional processing.
Mesial temporal sclerosis symptoms include the following:
- Strange sensations, such as auras, euphoria, déjà vu, jamais vu, or fear
- Changes in behavior/emotions
- Muscle spasms
- Temporal Lobe Epilepsy
- Seizures
The exact cause of mesial temporal sclerosis is still unclear. Some cases can result from injury to this part of the brain from prolonged febrile seizures. In other cases, a genetic susceptibility can play a role as well especially in cases where family members have had similar seizures. Other causes are related to viral infection and encephalitis, due to viruses such as human herpes virus type 6 (HHV-6), or to autoimmune disease where the immune system makes proteins that can attack the brain. Prolonged seizures and status epilepticus can also cause damage to the temporal lobe and induce MTS in patients with different other types of epilepsy.
Learn More:
Contact Our HelplineWhat Types Of Seizures May Be Seen?
Mesial temporal sclerosis is associated with focal seizures. These can present as tonic-clonic seizures or focal seizures with and without impaired consciousness.
Seizures often begin with feeling of a rising sensation in the stomach and throat, feeling sick to ones stomach, fear or anxiety, pause in behavior (behavioral arrest), Déjà vu (feeling of familiarity of the situation as if it happened before), jamais vu (feeling of unfamiliarity) or rarely an abnormal and unpleasant taste or smell. These are symptoms that are typical in focal seizures without loss of awareness.
- When the seizure evolves into a focal seizure with loss of consciousness, motor features can present with abnormal twisting motions of the hand or with automatic movements like hand picking or fumbling, or mouth chewing and lip smacking.
- Some seizures can evolve to a generalized tonic-clonic seizure.
- Because the seizures can involve language and memory areas, the seizures are often associated with inability to recall having had a seizure and with a transient inability to speak or inability to understand language during and shortly after the seizure.
How Is MTS Diagnosed?
The diagnosis of mesial temporal sclerosis includes detailed history and physical examination. A history of a prolonged seizure with fever in early life can be a risk factor for development of MTS.
- The MRI shows characteristic abnormal signal in the deep structures of the temporal lobe with scarring.
- Neuropsychology testing will often reveal signs of the disturbed function of the temporal structures, such as poor memory function or psychiatric disorders like depression and anxiety.
- Electroencephalography (EEG) shows epileptiform discharges, an excess electrical activity seen with epilepsy, in the region where the temporal lobe is located.
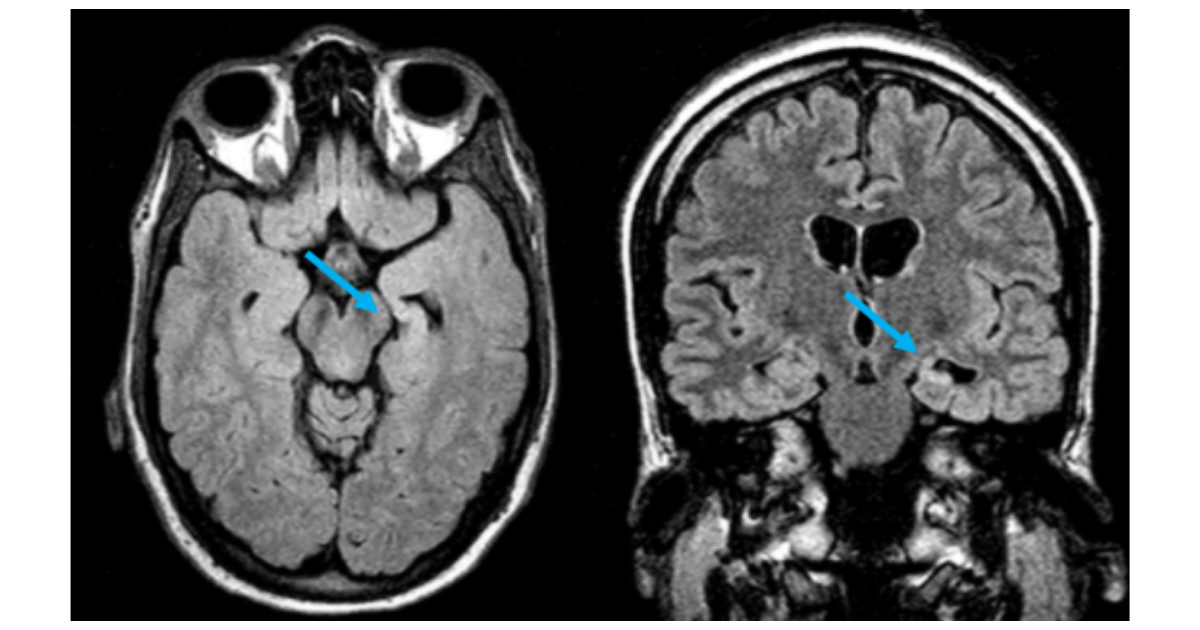
Figure: This MRI shows left mesial temporal sclerosis with a small and bright hippocampus with loss of internal structures.
Learn More
Find Your Local Epilepsy FoundationHow Is MTS Treated?
Medications
The first line treatment are antiseizure medications. There is no evidence that any one medication is most effective. If the first medication fails to control seizures, a second medication is typically tried. If two medications have not worked to stop seizures at good doses, seizures are considered drug-resistant, as further medicines are unlikely to be successful.
Other Treatments
If two medications have not worked, it is recommended that patients be referred for possible surgical evaluation. If MTS is only found on one side of the brain, then surgical resection is probably the best option in controlling the seizures. There are multiple options for surgery, ranging from minimally to more invasive options.
Minimally invasive techniques involve laser interstitial thermal therapy (LITT) which uses a small laser probe 2 mm in diameter which is inserted through a tiny hole in the skull to the area of MTS under direct MRI guidance. The laser heats the region and destroys the area of scarring, and the probe is then removed. The recovery after laser ablation surgery is rapid – most patients are able to leave the hospital the following day. Approximately, between 55% and 65% of patients become free of disabling seizures (that is focal seizures with loss of awareness or GTC seizures) after a follow-up period of one to two years. Because it is a relatively new procedure and the follow-up periods are limited to 2 years in most reports, it is too soon to know how its success compares to that of temporal lobe resections, which are more invasive procedures.
More invasive options include opening the skull to resect an area of the temporal lobe. In some cases, the anterior portion of the temporal lobe is resected, whereas in other cases, a more selective resection of the hippocampus and amygdala are performed.
"It is important to talk with your doctors to determine which option is the best for you."
If MTS involves both sides of the brain then surgical resection is often not possible, as one cannot remove both temporal lobes due to memory and other functional concerns. In such cases, responsive neurostimulation (RNS) is often considered. RNS involves a device that involves wires and/or strips implanted inside the temporal lobe affected by MTS. This device records brain activity continuously and when it detects a seizure starting, it delivers a small electrical discharge to try to stop the seizure. This device can also provide information on the proportion of seizures that arise from the left vs the right side. If after one year, the majority of the seizures are found to originate from one side, a palliative resection can be considered. A palliative resection means that seizures will not be completely stopped after surgery but can be reduced.
Other treatment options for MTS are vagus nerve stimulation (VNS) which involves implanting a stimulator device in the chest and connecting it to the vagus nerve in the left side of the neck. The device will deliver electrical impulses to the brain through the nerve to modulate the seizure activity.
Another type of stimulator is the deep brain stimulation (DBS) device. This device involves wires that are placed into a region of the brain called the thalamus, which is a deep nucleus in the brain that works as a hub that connects different brain regions. Stimulation modulates activity and can decrease seizures.
What Is the Outlook?
Seizures may initially be responsive to antiseizure medications but over time, they often recur, and become poorly controlled in most cases (60-90%). Many of these cases who respond poorly to medication can do very well, and often become seizure free with surgery.
Many patients have challenges with memory, as well as have higher rates of depression and anxiety. When patients become seizure-free, their memory can start to improve. Many persons will respond well to medications or other therapies for mood disorders. Paying attention to these non-seizure symptoms of epilepsy associated with MTS is crucial.
Learn More:
Donate to Support Our MissionResources
Epilepsy Centers
Epilepsy centers provide you with a team of specialists to help you diagnose your epilepsy and explore treatment options.
Epilepsy Medication
Find in-depth information on anti-seizure medications so you know what to ask your doctor.
Epilepsy and Seizures Helpline
Call our Epilepsy and Seizures Helpline and talk with an epilepsy information specialist or submit a question online.
Tools & Resources
Get information, tips, and more to help you manage your epilepsy.
Related Stories

Press Releases
Epilepsy Foundation of America Awards $250,000 at 14th Annual Shark Tank Competition
Read Story
Press Releases
Joyce A. Cramer to Receive Lifetime Accelerator Award for Transformative Contributions to Clinical Research and Epilepsy Innovation
Read Story